
The governments have recognised that the health care system needs to have equity of access. This means that health care is easily accessible when needed and equitably distributed amongst the population. The nature of Australia’s population distribution across such a large land mass makes equity of access to health facilities and services difficult. Most Australians live in metropolitan areas and have readily available access to health facilities and services.
Disadvantaged Groups
This is not the same for people living in rural and remote areas who have less access to health facilities and services. This includes limited access to hospital services, especially a lack of private hospitals, and specialist services. In order to address this inequity of access to health facilities and services the government has instituted services such as the Royal Flying Doctors, e-Health records and Telehealth technology to provide access to specialists and other services via video conferencing.
ATSI also have poorer access to health facilities and services. They have less access to dentists, general practitioners, and hospitals. The barriers included things such as: long waiting times, cost, unavailable services, and culturally inappropriate services.
People with lower levels of education also have less access to health facilities and services, as this can limit their knowledge regarding their health needs and ability to navigate the system.
A few stats for evidence
- Cost hindered 2.4% of people from seeing a GP, 14.8% from seeing a dentist, and 5.8% from seeing a medical specialist. The % is higher for people on the lower end of the socioeconomic scale (e.g. 20% delay in dentistry compared to 9%)
- 16.6% of people waited longer than thought acceptable to see a GP.
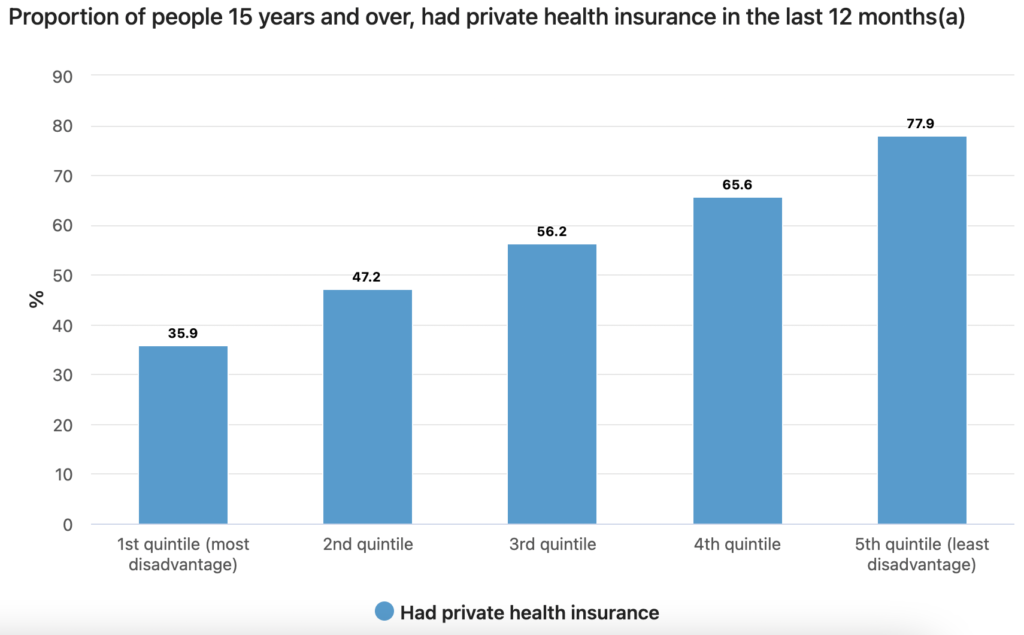
- 45.5% of Australians have private hospital cover, and 54.6% have ancillary cover (extras), such as dentistry and optometry. Only 35.9% of people living in high socio-economic disadvantage had private health insurance compared to 77.9% from the least disadvantaged.
What the government is doing
The biggest action by the government for equity of access to health facilities and services was the introduction of Medicare and the Pharmaceutical Benefits Scheme. This has greatly removed cost as a barrier to a number of health facilities and services, but not all. Health services such as dentists, physiotherapists, psychologists or occupational therapists are not covered by Medicare, which results in inequitable access to these services.
Local Hospital Networks is another example of the government working to improve equity of access to health facilities and services. LHNs are groups of hospitals that link services within a region or specialist networks in the state or territory. This increases local autonomy and flexibility to respond to local needs.